The Share & Care Foundation, along with our Healthcare to Unreached Signature Program local partners, continue the fight toward reversing the healthcare challenges facing today’s marginalized poor.
Our focus is and has always been on prevention. We do this by supporting programs that are repeatable — that is, they have been created (and documented) with the intention of improving over time for use in other populations with similar needs. While funding is also needed for one-time disaster recovery efforts, our approach is about investing in people to create permanent change. We do this by addressing the absence of what we call the the five A’s:
- Affordable healthcare.
- Accessible resources.
- Awareness of good health practices.
- Accountability of healthcare providers.
- Available healthcare facilities.
Healthcare is a basic human right. Let’s take a look at how we’re bringing healthcare to marginalized populations across Rajasthan, Gujarat, Maharashtra, Tamil Nadu, and Manipur.
Thar Desert, Rajasthan
Program: Nutrition & Health for Women & Girls

Our journey begins in Rajasthan, where we are focusing on nutrition and health for women and children living in five Thar Desert villages.
Life in the Thar Desert is difficult. Food sources are limited, there is no continuous supply of water, and families live together in large groups, all of which contribute to the spread of diseases and ultimately, high mortality rates.
Thar Desert Challenges
Nutrition
Across India, the number of children and women (pregnant and non-pregnant) with anemia hovers just above 50%, and given the extremely poor health conditions of the Thar Desert, the rate is higher and has had a significant impact on its residents. This is in spite of the fact that routine screening — which doesn’t require complicated expertise — is the best prevention.
The other nutrition-related challenge they’re facing is diabetes. Rural rates of diabetes are at around 3%, with urban rates even higher (around 9%), which means India currently has the highest number of diabetics — 40 million — of any one country in the world.
Sexual and Reproductive Health
There are many cultural and religious taboos around menstruation for girls and women, particularly among largely tribal populations in rural, isolated areas like the Thar Desert. Because of this, girls aren’t able to learn about what’s going on with their bodies as they mature, as often their mothers don’t understand the biological reasons herself. Even in schools, teachers find it too embarrassing to talk about openly. So women and girls live in silence and shame, with little or no sources to learn proper sanitation practices.

Mental Health
As with sexual health, mental health is rarely discussed, much less understood. When a woman gives birth and finds herself depressed, as with postpartum depression, it goes undiagnosed and untreated. Dementia in older women, and men, is also misunderstood. Bringing mental health issues out into the open is needed to ensure no one has to endure something that may very well be treatable.
Our Vision
We’ve done a lot of work in this region historically, with a goal of creating a holistic path to better health and nutrition that can be replicated in additional Thar Desert villages. Village health workers are key to bringing change to this region, and play a vital role in our overall village upliftment programs.

Specifically, we are working to deliver life-saving nutrients and to educate and raise awareness to benefit 5,000 women and children across five villages:
- Provide necessary nutrition supplements, horticulture practices, and education on ongoing prevention of anemia and diabetes.
- Help women and girls understand their menstrual health and the importance of hygiene, including providing the necessary supplies. Boys too need to understand their journey through puberty and overall reproductive health.
- Educate and reverse upward trends of noncommunicable disease inherent in poor populations, largely caused by tobacco use, physical inactivity, alcohol abuse, and unhealthy diets.
- Address mental health issues through education and treatment.
Saurashtra, Gujarat
Programs: Anemia Prevention, Diagnosis & Treatment; Maternal, Newborn & Child Health in Tribal Areas; Cancer Prevention
 Heading 500 miles to the south, our on-the-ground work is focusing on the issues affecting women and children across 600 villages in the state of Gujarat that includes scarce government services, a shortage of doctors and other health professionals, and poor local governance.
Heading 500 miles to the south, our on-the-ground work is focusing on the issues affecting women and children across 600 villages in the state of Gujarat that includes scarce government services, a shortage of doctors and other health professionals, and poor local governance.
Challenges
Social
Social issues include alcoholism and other drugs, education and access to family planning tools (e.g., contraceptives), and violence toward women.
General Health
Malnutrition and anemia affect around 70% of children in Saurashtra. Other health issues include gastrointestinal disorders (e.g., dysentery, parasitic infections), and a higher-than-average level of genetic disorders, such as sickle cell anemia.
Tribal areas also have higher mortality rates overall.

Infant Mortality
While infant, maternal, and child mortality rates are of great concern, the rate of postneonatal mortality (neonatal is the first 28 days of life, postneonatal is between 28 days and one year) illustrates some of the disturbing underlying issues:
- 41% of infant deaths are post-neonatal (28 days–1 year)
- 55% of those are from sepsis and pneumonia
- 70% of those occurred at home
- 77% of those sought care
- 35% of those were admitted to a healthcare facility
In addition, miscarriages and abortions are higher among tribal women, with low birth weight topping sepsis and pneumonia as the leading causes of neonatal deaths. There’s also evidence that maternal morbidity and delayed breastfeeding are associated factors.
Cancer
Rates of cancer are rising among tribal communities, with more than two-thirds of cases in women. While most cases are associated with tobacco, low physical activity, and an unhealthy diet, it’s the lack of awareness and knowledge of these health factors that’s particularly lacking.
Our Vision
Malnutrition and Anemia
As with nearly all the locations we serve, malnutrition and anemia are rampant and are being addressed by providing the necessary nutrition supplements as well as education on ongoing prevention.

Infant Mortality
Infant mortality — and maternal, newborn, and child health in general — are being addressed through community-based technology. This is a program we’ve supported in many locations, including ongoing improvements to coverage.

Originally created by the government in 2005, and used in tribal villages since 2013, accredited social health activists, known as Ashas, use mobile phones and a proprietary application to bring health services directly into homes.
Innovative Mobile Phone Technology for Community Health Operations — or ImTeCHO — gives trained Ashas the ability to:
- Stay on top of scheduling and tasks associated with home visits.
- Share educational videos and multimedia presentations to assist in educating patients on their condition and care.
- Present diagnosis and customized treatment plans based on observation and a predetermined set of questions.
- Support immediate care through real-time interaction with medical experts at remote locations.
- Help families manage infant care through a care model coordinated by a remote infant care center.
Infant — and child — mortality is also being addressed through a program referred to as SNCU, or special neonatal care unit, which is a follow-up program designed to lower out-of-hospital death rates among children and premature babies with low birth weight. The program includes ensuring the children are carefully monitored for nutritional health and other childhood illnesses, and that they receive all appropriate immunizations.

We currently have 584 children in the program, who receive regularly scheduled home visits and examinations (including collecting valuable health data) through to their second birthdays. So far, the percentage of discharged newborns and infants who were later visited at least once at their homes is 94.8% — a very promising number!
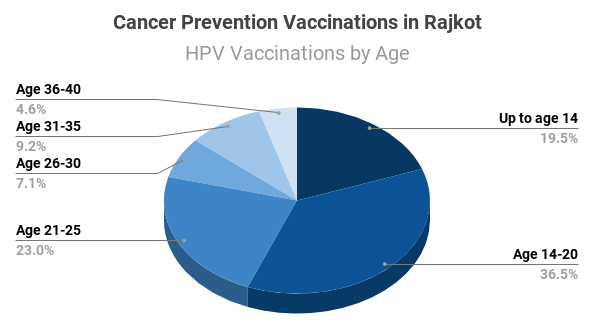
Cancer
The most effective first steps toward reducing cancer and cancer deaths is early diagnosis. To that end, we are supporting screening tests designed to identify malignancies at their earliest stages.
To combat cancer over the long term — particularly those related to smoking and obesity — education, awareness, and vaccinations are other key components of the project. To reach as many people as possible, educational events are being set up at schools, colleges, and other community centers. Doctors, other medical professionals, and volunteers will arrange interactive “camps,” complete with on-site checkups and educational materials such as videos, presentations, and other visual and hands-on teaching tools.
Our goal for this project is to reach 100,000 people through awareness programs and checkups, including 5,000 women screened for breast and cervical cancer, and 2,000 girls vaccinated for HPV, or human papillomavirus, which can cause various cancers later in life.
And, in line with our core philosophy of supporting repeatable programs, all records are being carefully maintained to ensure ongoing program improvements and oversight.
Nanded, Maharashtra
Program: Mobile Unit: Save Life at Birth
Traveling another 700 miles southeast to Nanded in Maharashtra, we are bringing a comprehensive community health program to 25 villages to address local challenges in family planning, mother and child health, disease, malnutrition, and dehydration.
Our Vision
What sets this program apart is incorporating a community organizer and Dai — or “birth attendant” — into village life. The organizer and Dai report to a nutritionist-educator, who in turn reports to a field staff support team.
To address the challenges inherent in village life, the program is based on education and works within a training-reporting-monitoring system with the goal of preparing mothers to take full responsibility for their and their child’s health and nutrition, including:
- Family planning
- Self-care during pregnancy
- Immunizations
- Food prep and low-cost nutrition
Thiruthuraipoondi, Tamil Nadu
Program: Pregnancy & Maternal Care for Landless Labor Communities
Next we travel nearly 800 miles farther southward to Thiruthuraipoondi block in Tamil Nadu. There, 100 women across 870 villages (within Thiruvarur district) are part of a program addressing the socio-demographic factors affecting a crucial period in their lives: pregnancy.
Challenges
Nearly 80% of the population of Thiruthuraipoondi block (and Thiruvarur district) is rural. Due to the challenges of poverty and a lack of accessible modern healthcare facilities and nutritional care (to name just a fraction of causes), this area suffers from many of the same problems as other rural populations, including malnutrition, anemia, and low birth rate, but also pediatric HIV infection.
Our Vision
For the sake of the mother and child’s health — as well as that of future generations — the program focuses on the challenges of poverty and access to facilities.
Most importantly, each woman receives a full two years of support beginning when she first learns she’s pregnant. Comprehensive support begins with a stress-free pregnancy, and also includes delivery assistance, monitoring developmental milestones for the baby, and medical and nutritional support.
For women who would otherwise have little to no access to the real care they and their baby need, this program can change their lives, and those of their children.
Kangpokpi and Imphal West, Manipur
Program: Rural Health in Imphal, Manipur: Essential Healthcare for the Underserved
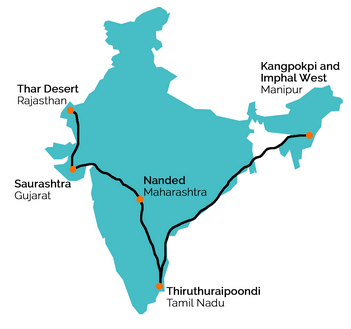
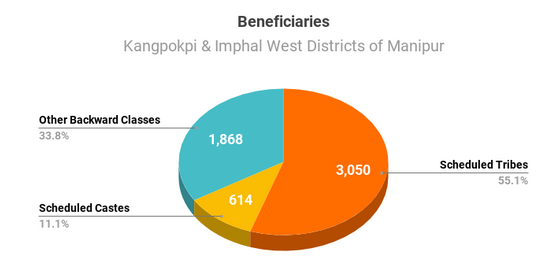
Now we head more than 2,000 miles northeast, the longest leg of our journey, to five villages in the Kangpokpi and Imphal West districts of Manipur. Here we’re providing ongoing essential health services to the most neglected population — children and women — within an also-neglected population consisting mostly of Scheduled Tribes, Scheduled Castes, and Other Backward Classes.
Challenges
Just under half of the 5,532 villagers are considered marginalized (2,648), including children, pregnant women, and nursing mothers, and are in need of basic healthcare, education and awareness of proper hygiene practices, antenatal and postnatal care, and COVID-19 protocols, among other health concerns.


Our Vision
Free treatments and medicines are being distributed to 2,648 marginalized children and adults.
By providing care through clinic visits and a Mobile Medical Clinic, mothers are receiving the specialized antenatal and postnatal care needed to better ensure healthy children as well as healthy moms. To prevent unwanted pregnancies, eligible couples receive supplies and education on the use of condoms and other contraceptives. And for all — children and adults — essential vaccinations help prevent and fight infections faster and more effectively.
Education is always an essential part of the work we do. Clinic staff are hosting monthly educational meetings — complete with multimedia teaching tools — to teach good hygiene and health practices.
During this time of the ongoing pandemic, COVID-19 protocols are also part of our educational outreach. To reach more people, and to minimize spread of the virus, we are also going door-to-door.

At the time of this writing, 1,556 villagers have received COVID-19 awareness and prevention training, 450 households have received home visits, 1,800 villagers have received face masks, sanitizers, and soaps, and 296 needy families have received groceries.


As we near the end of the “year of the pandemic,” we are grateful for the opportunity to be useful and to bring awareness that we believe will help change lives for generations to come. healthcare is necessary to form a strong foundation for populations that need to be recognized as equal to us all.
But we can’t do it alone, we rely on people like you to share in our determination to rid the world of the inequities that continue to alienate those born into poverty and denied their rights to education and basic healthcare. A gift in an amount affordable to you will make a world of difference to so many.